Which is Better for Lupus Nephritis: Benlysta or Lupkynis?
NOTE: Johns Hopkins University Press, publisher of The Lupus Encyclopedia, is a nonprofit publisher. If you purchase JHUP books, like The Lupus Encyclopedia, you support projects like Project MUSE.
Which is better for lupus nephritis? Benlysta or Lupkyinis? … and the winner is… (read below)
Updated 6/1/21: This post now includes:
The specifics on the complete renal responses for Benlysta vs Lupkynis.
Information on extra-renal lupus.
Details about the long-term extension trial to 104 weeks with Lupkynis.
Background on Lupus Nephritis (LN)
Systemic lupus erythematosus (SLE) is an autoimmune disease where the immune system attacks the person’s own body. Around 40% of the time, it will attack the kidneys. This condition is known as lupus nephritis (LN).
Unfortunately, lupus nephritis causes no symptoms whatsoever until it is severe and permanent damage is already occurring. Consequently, this is why we ask our SLE patients to give a urine sample every 3 months to look for increased protein in the urine (proteinuria) as an early sign of nephritis.
Up until recently, our treatments have not been very good. Historically, around 15% of patients went into kidney failure within 10 years of their diagnosis, eventually needing dialysis or a kidney transplant. “Standard of care” with mycophenolate and cyclophosphamide are simply NOT good enough.
Our ultimate goal in treating LN is to achieve remission. Over the past decade, numerous drugs have been studied to find better treatments. In those studies, only 22% to 32% of patients went into remission on the usual treatments. Because remission is the best way to prevent kidney failure and death, finding better therapies is crucial.
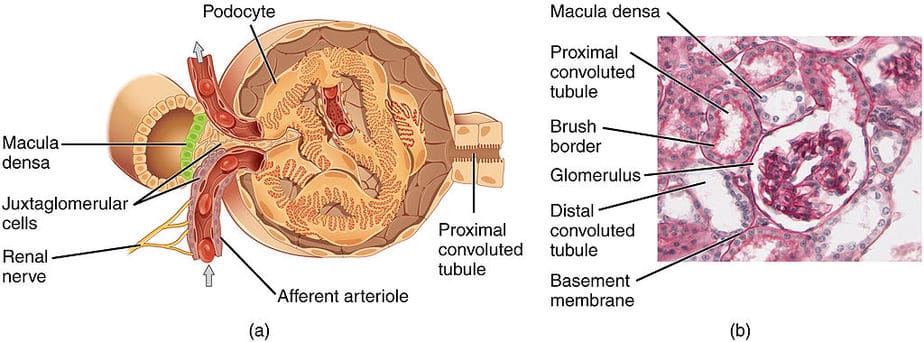
A normal nephron in the kidney (glomerulus). We have millions of these filters. Photo by OpenStax College from wikipedia.com
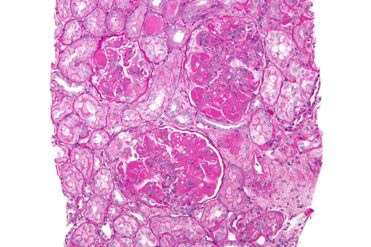
Lupus class IV (diffuse proliferative nephritis). Photo by “nephron” at wikipedia.com
The Role of the Kidney Biopsy in Lupus Nephritis
A kidney biopsy is essential to help rheumatologists figure out the best course of action. After numbing the back under the ribcage, a tiny needle is inserted to grab a small tissue sample, which is then examined under a microscope.
Normal Kidney: Note the normal kidney in the top right image. The glomerulus (nephron) is one of millions of tiny filters in our kidneys. The white spaces are essential for waste products to fill up and flow into the urine.
Lupus Nephritis Kidney: Now look at the LN kidney on the bottom, which is affected by the worst form called “class IV diffuse proliferative nephritis.” Notice how there are hardly any large white spaces left. Because this filter is unable to remove waste products, the patient would absolutely go into complete kidney failure without good treatment.
The FDA is responsible for evaluating the safety and effectiveness of new drugs. Photo from Wikipedia
Recent FDA Approvals for Lupus Nephritis
Prior to 2020, there were no FDA-approved drugs specifically to treat LN. However, that recently changed:
December 17, 2020: Benlysta (belimumab) became the 1st FDA-approved drug to treat adults with lupus nephritis when added to standard of care (high doses of steroids plus either mycophenolate or cyclophosphamide).
January 21, 2021: Lupkynis (voclosporin) became the first oral drug FDA-approved to treat adults with LN when added to standard of care (high dose steroids plus mycophenolate).
May 5, 2021: Benlysta was officially approved to treat adults with LN in the European Union.
So, Which is Better: Benlysta or Lupkynis?
To determine which medication is better for lupus nephritis, we must look at the pros and cons of both drugs side-by-side.
Benlysta (belimumab) Overview
Data below is from the phase III clinical trial (BLISS-LN) unless otherwise stated.
Benlysta: Key Advantages and Safety
Flexible options: Given either by IV (intravenous) by a nurse or at home by self-injection (SQ form).
Proven Track Record: Has been used since March 2011, providing extensive experience regarding its safety and effectiveness. Safety in LN trials was similar to phase III SLE trials.
Accessibility: You do not have to fail other drugs first before using it for LN.
Steroid Sparing: Steroids had to be tapered to 10 mg a day or less of prednisone by week 24.
Comprehensive Care: Proven safe and effective for systemic lupus problems other than kidney inflammation (arthritis, skin lupus, high anti-dsDNA, low C3/C4).
Pediatric Use: FDA-approved to treat children with SLE as young as 5 years old.
Support: Excellent patient assistance program at www.benlysta.com.
Clinical Efficacy (104 Weeks)
Response Rates: Complete renal response (CRR) at 104 weeks was 30% on Benlysta (plus MMF or cyclophosphamide + steroids) versus 20% on standard of care alone.
The Odds Ratio: The odds ratio for CRR was 1.74 (74% greater odds). Note: The Benlysta trial used a stricter definition for CRR than the Lupkynis trial.
Sustained Response: Patients had a 58% increased likelihood of achieving and remaining in CRR until week 104.
Long-term Outcomes: Resulted in a 49% lower likelihood of a “renal-related event or death” up to week 104.
Benlysta: Considerations (CONS)
Injections: People who do not like needles may find it difficult.
Representation: Only around 14% of patients were Black (under-recruitment remains an industry problem).
Cost: Expensive, though generally less so than Lupkynis (estimated at $43,000/year).
Lupkynis (voclosporin) Overview
Data below is from the phase III clinical trial (AURORA trial) unless otherwise stated.
Pros and Mechanism
Oral Form: Capsule form; no injections required.
3rd Generation CNI: More potent than cyclosporine and less likely to cause cholesterol issues or diabetes compared to tacrolimus. Stable drug levels mean routine blood monitoring isn’t required.
Direct Kidney Protection: Stabilizes podocytes (essential filter cells) in addition to providing immunosuppression.
Steroid Taper: Amazing taper! Starting at just 25 mg/day (after 2 days of IV SoluMEDROL) and reaching 2.5 mg by 4 months is phenomenal.
Clinical Efficacy (52 to 104 Weeks)
Response Rates: CRR at 52 weeks was 41% (plus MMF/steroids) versus 23% on standard of care.
The Odds Ratio: 2.7 (170% greater odds of achieving CRR).
Speed of Treatment: Achieved low urine protein twice as fast (172 days vs 372 days). “Time is kidney!”
Diverse Patient Outcomes: Black patients saw excellent results; 46% achieved CRR by 1 year compared to just 16% on standard of care (nearly 3x more effective). Hispanic patients also saw 39% achieving CRR at 1 year.
Considerations (CONS)
Pill Burden: Most commonly 3 capsules taken twice daily.
Side Effects: Decreased kidney function and high blood pressure are common for CNIs, though studies showed no meaningful mean eGFR difference vs placebo by week 52.
Monitoring: Blood pressure and kidney function need checks every 2 weeks for the first month, then monthly.
Limitations: Not FDA-approved for non-renal SLE; studied only with MMF (not cyclophosphamide); not recommended for pregnancy/breastfeeding.
The Complete Renal Response (CRR) Criteria Explained
Why is a complete renal response (CRR) so important? Our goal in treating lupus nephritis is remission. Patients who reach remission are much less likely to go into kidney failure, suffer less organ damage, and live significantly longer.
While “CRR” is not officially called “remission” (because true remission requires a follow-up kidney biopsy), it is the closest clinical measure we have.
What did the Benlysta and Lupkynis studies have in common?
Neither study allowed significant increases in steroids, changes in blood pressure medicines (ACEi’s/ARBs), or the addition of other immunosuppressants. Both studies also had a very similar urine protein to creatinine ratio (UPCR) goal: around 0.5 mg/mg or less.
The big difference was in the kidney function stabilization criteria:
Medication
Required eGFR for Complete Renal Response
Benlysta
90 ml/min or higher (or within 10% of the baseline if less than 90).
Lupkynis
60 ml/min or more (or within 20% of the baseline if less than 60).
It is significantly more difficult to maintain an eGFR of 90 ml/min or higher when you have severe lupus nephritis, making Benlysta’s requirement very impressive. However, Lupkynis balanced this by using CRR as its primary endpoint, whereas Benlysta used it as a secondary endpoint.
Important Fact About Lupkynis and Pregnancy
Other calcineurin inhibitors (such as tacrolimus) are safe to use in pregnancy. Therefore, why is Lupkynis not recommended during pregnancy?
Each capsule of Lupkynis contains 21 mg of alcohol. To put that into perspective, 5 oz of red wine contains around 4000 mg of alcohol. However, the Centers for Disease Control explicitly states: “There is no known safe amount of alcohol use during pregnancy or while trying to get pregnant.”
The Verdict: Benlysta vs Lupkynis
Neither is definitely any better or worse than the other!
Ultimately, they are both game-changers in the treatment for lupus nephritis, and they both have their vital place in rheumatology.
What Are the Next Steps for Severe Lupus Nephritis?
The main problem with older LN treatments is that most patients do NOT go into remission quickly enough. While waiting for standard therapies to work, permanent damage occurs. Once you lose a nephron due to lupus inflammation, it is gone forever.
Furthermore, older treatments rely heavily on high doses of steroids, which inevitably cause significant side effects and long-term organ damage.
With Benlysta and Lupkynis, we now have two drugs proven to increase remission rates, work faster, and decrease the need for steroids. In my medical opinion, they are markedly safer than long-term high-dose steroids.
For lupus nephritis, I recommend immediate treatment with Benlysta OR Lupkynis, combined with mycophenolate, hydroxychloroquine, an ACE inhibitor (or ARB), Vitamin D, and religious sunscreen usage.
If my nephritis were severe, I would also explore if my insurance would cover both Benlysta and Lupkynis at the same time. Because they work through two different mechanisms, combining them could theoretically achieve remission and taper steroids even faster.
What Should You Do If You Have Lupus Nephritis?
Learn as much as you can. Knowledge is power!
Accept your medication regimen. You will need to take numerous medications. When pill fatigue sets in, remind yourself: “I want to do everything possible to stay off dialysis and prevent needing a kidney transplant.” Let your medications do their magic so you can taper off the damaging steroids.
Consider Benlysta if: You seek an easy-to-take medicine with proven long-term safety.
Consider Lupkynis if: You prioritize potentially faster results and can tolerate six daily capsules along with frequent blood monitoring.
For the most aggressive approach: Ask your doctor about combining both medications to give your kidneys maximum protection.
For More In-Depth Information on Lupus Nephritis
Read chapters 12 and 34 of The Lupus Encyclopedia, edition 2. You can also look up your symptoms, conditions, and medications in the index.
If you have lupus nephritis, what has your experience been? What do you recommend for other patients? Do you have any questions for Dr. Thomas?
Please click on “Leave a Comment” above to join the conversation.
References
Package inserts for both Benlysta and Lupkynis.
Furie R, Rovin BH, Houssiau F, et al. Two-Year, Randomized, Controlled Trial of Belimumab in Lupus Nephritis. N Engl J Med. 2020 Sep 17;383(12):1117-1128.
Kuglstatter A, Mueller F, Kusznir E, et al. Structural basis for the cyclophilin A binding affinity and immunosuppressive potency of E‐ISA247 (voclosporin). Acta Crystallogr D Biol Crystallogr. 2011;67(pt 2):119‐123.
Bîrsan T, Dambrin C, Freitag DG, et al. The novel calcineurin inhibitor ISA247: a more potent immunosuppressant than cyclosporine in vitro. Transpl Int. 2005;17(12):767‐771.
Mayo PR, Huizinga RB, Ling SY, et al. Voclosporin food effect and single oral ascending dose pharmacokinetic and pharmacodynamic studies in healthy human subjects. J Clin Pharmacol. 2013;53(8):819‐826.
Gibson K, Parikh S, Saxena A, et al. AURORA phase 3 study demonstrates voclosporin statistical superiority over standard of care in lupus nephritis. National Kidney Foundation virtual 2020 Spring Clinical Meetings; March 26‐29, 2020.
Arriens C, Polyakova S, Adzerikho I, et al. AURORA phase 3 study demonstrates voclosporin statistical superiority over standard of care in lupus nephritis. EULAR European E‐Congress of Rheumatology 2020; June 3‐Sept 1, 2020.
Askanase A, Randhawa S, Lisk L, et al. Efficacy of voclosporin across lupus nephritis biopsy classes. National Kidney Foundation virtual 2021 Spring Clinical Meetings; April 6‐10, 2021.
Rovin BH, Parikh SW, Huizinga RB, et al. Management of lupus nephritis with voclosporin: an update from a pooled analysis of 534 patients. American Society of Nephrology Kidney Week 2020 Reimagined; Oct 19‐25, 2020.
Caster DJ, Solomons N, Randhawa S, et al. AURORA phase 3 study demonstrates voclosporin statistical superiority over standard of care in lupus nephritis. ERA‐EDTA Virtual Congress; June 6‐9, 2020.
DISCLAIMER: I am on the Speaker’s Bureaus for both Benlysta and Lupkynis. I do this proudly as I believe strongly in how much these medications can improve the treatment of our lupus patients, helping them live longer, better lives. I hope you can agree that the information I presented above is unbiased, using the data from the research studies. However, the opinions expressed in what I would want for treatment and what I recommend for patients are my opinions, based upon the research results.
For more in-depth information on Lupkynis vs Benlysta for Lupus Nephritis: Dr. Thomas Has His Verdict!:
I have some cons to include/add to Benlysta (IV) at an infusion center…. it takes time to be infused. From start (vitals, questions, pre meds, iv placement, blood drawn for blood work, saline, pharmacy mixing meds) and the hour of actually being infused it is two hours on the short side. On a bad day it could be closer to four hours due to staff shortage, pharmacy back up, poor scheduling, over crowding at the center (beyond capacity due to closing for holidays, snow storms or any number of things like the Charlottesville riot).
Can you provide additional detail on the difference in criteria for a complete renal response between the two studies? Stricter, sure, but how much stricter?
Bo: Sorry for the delay in my response. I’ll include this information in the blog post as well.
First, what did they have in common? – Both did not allow any significant increase in steroids, change in doses of ACEi’s or ARBs, addition of an antimalarial if not on one already, and no addition of any other immunosuppressant drug.
The other is they both had a similar urine protein to creatinine ratio (UPCR) goal (with one slight, nonsignificant difference). Lupkynis patients had to reach a UPCR of 0.5 mg/mg or less; Benlysta patients had to be below 0.5 mg/mg.
The big difference was in the kidney function stabilization criteria. Benlysta required a eGFR of 90 ml/min or higher (or within 10% of the baseline if less than 90), while Lupkynis patients could have a eGFR of 60 ml/min or more (or within 20% of the baseline if less than 60). It is much more difficult to have an eGFR of 90 ml/min or higher when you have severe lupus nephritis. So, this was an impressive requirement.
However, this is balanced by Lupkynis using the CRR as its primary endpoint, while Benlysta used it as a secondary endpoint. Having it as the primary endpoint is wonderful as that is truly our goal. We don’t just want a “renal response,” with a treatment, we want remission (CRR or close to a CRR).
Thanks for this important question
Hello, 2 year data is now available for Lupkynis (See EULAR readout)… It was extremely well tolerated over the duration and had additional efficacy benefits. 3yr readout will be available some time next year, but for now Lupkynis is demonstrated to be tolerated well for the same duration as Benlysta.
Sam: Yes, I heard the same. Thus far, all we could say is that it is safe and effective for 52 weeks (the number of weeks in the phase 3 clinical trial). However, we usually use lupus nephritis therapies much longer than that. I cannot wait for the data to be published so I can review it.
[…] Lupus Patients Need to Know About Lupus Nephritis Urine Samples nephritis – How it is diagnosed – The importance of diet, exercise, mindfulness – How it is treated – What happens when it is not treated – How to get the most out of virtual online doctor visits […]
[…] Benlysta Reviews: Learn the amazing truth on how it works first infusion or self-injection, make sure to learn as much as you can from this and other Benlysta reviews. Today, we use Benlysta for lupus nephritis, SLE, and pediatric […]
I would be very interested in your opinion as to whether or not you recommend adding Benlysta or Lupkynis for your patients who have a history of nephritis and are on mycophenolate, plaquenil, and an ACE or ARB but are currently stable or “in remission”.
Thank you
Ann: Once we find a combo that has someone in remission, we like to stay there. Many of us now recommend after 3 years of lupus nephritis remission… getting another kidney biopsy. If no inflammation… then see if we can slowly taper off the mycophenolate. REASON: Some patients look like they are in remission, but really are not. If mycophenolate is tapered without knowing this, they are the ones who are at high risk of flaring… then you are looking at more steroids and probably increased kidney damage. This comes form the work of Dr. Brad Rovin at OSU. Have a Merry Christmas! … Donald Thomas, MD
Dr. Thomas, I am a now disabled academic internist with a 40-year history of lupus and nephritis. I’ve been on HCQ, Cellcept, and low-dose (4 mg) prednisone until last year when I had to stop HCQ due to apical CMP and arrhythmias. I had a renal flare in September after a bout of pneumonia, which responded to increased Cellcept. My anti-ds DNA is negative, but C4 is low, and I have intermittent arthralgias/arthritis. Would you recommend I add Benlysta at this time to avert flares and enable further prednisone (now at 6 mg daily) and Cellcept tapers (1500 mg total) dose? I developed recurrent zoster on Cellcept 2000 mg daily despite adequate prophylaxis and hx of Shingrix vaccination.
Thanks in advance!
Absolutely! The latest ACR guidelines for lupus nephritis recommend triple immunosuppressant therapy using either belimumab or a calcineurin inhibitor (voclosporin or tacrolimus) plus steroids from day 1 of the diagnosis with the plan of a quick taper off steroids. Reasoning… the vast majority of patients treated with older regiments (like mycophenolate ) do not achieve remission and every flare is associated with permanent loss of nephrons. ‘
The belimumab and voclosporin clinical trials demonstrated complete renal responses that were 2 to 3 fold greater than mycophenolate or cyclophosphamide alone.
Many of us even use BEL + a CNi + MMF as it helps to keep patients off steroids which are the #1 cause of side effects (even a low dose of tacrolimus 1 mg bid can have impressive and fast results).
Dr. Thomas , im writing because I this point I don’t know if I can take iv infusion benlysta and Lupkynis together my doctor for my kidney told me is ok to take together but my doctor who is the one is take care of my Lupus he told me I can’t do iv infusion and lupkynis together, im so confused im trying to research for information.
Angelina: I absolutely do use the combination with great success. Benlysta calms down the B cells; Lupkynis calms down the T-cells but also helps repair the filters of the kidneys called the podocytes and this effect is often very fast. With the combination (plus hydroxychloroquine), Ive been able to lower steroids a lot quicker and steroids is by far our most dangerous drug.
Dr. Thomas, it sounds as though you have had success with both lupkynis and benlysta together with celcept and plaq. How long do your patients benefit from taking lupkynis and benlysta together? Is it one to two years or ongoing?
After being in clinical remission for 3 years or more, I consider tapering off Lupkynis and CellCept (one at a time). However, I offer a kidney biopsy first to ensure 100% remission prior to tapering.
I recommend continuing both Benlysta and Plaquenil as they have both been shown to reduce the loss of kidney function and long term organ damage






Leave a comment